Some FODMAPs, such as fructose, are readily absorbed in the small intestine of humans via GLUT receptors. Absorption thus depends on the appropriate expression and delivery of these receptors in the intestine. Improper absorption of these FODMAPS in the small intestine leaves them available for absorption by gut flora. The resultant metabolism by the gut flora leads to production of gas and potentially results in bloating and flatulence.
The physiological basis for the genesis of many functional gut symptoms is luminal distension. Luminal distension not only induces the symptoms of pain, the sensation of bloating and visible abdominal distension, but may also lead to secondary motility changes. Thus, minimizing the consumption of dietary factors that can distend the intestine would theoretically lead to improvement in global symptoms.
Dietary components that lead to luminal distension are poorly absorbed in the proximal small intestine, will be small molecules (i.e. osmotically active), will be rapidly fermented by bacteria (with the potential to be fermented by small intestinal as well as cecal bacteria and to expand the bacterial population), and will be associated with hydrogen rather than methane production.
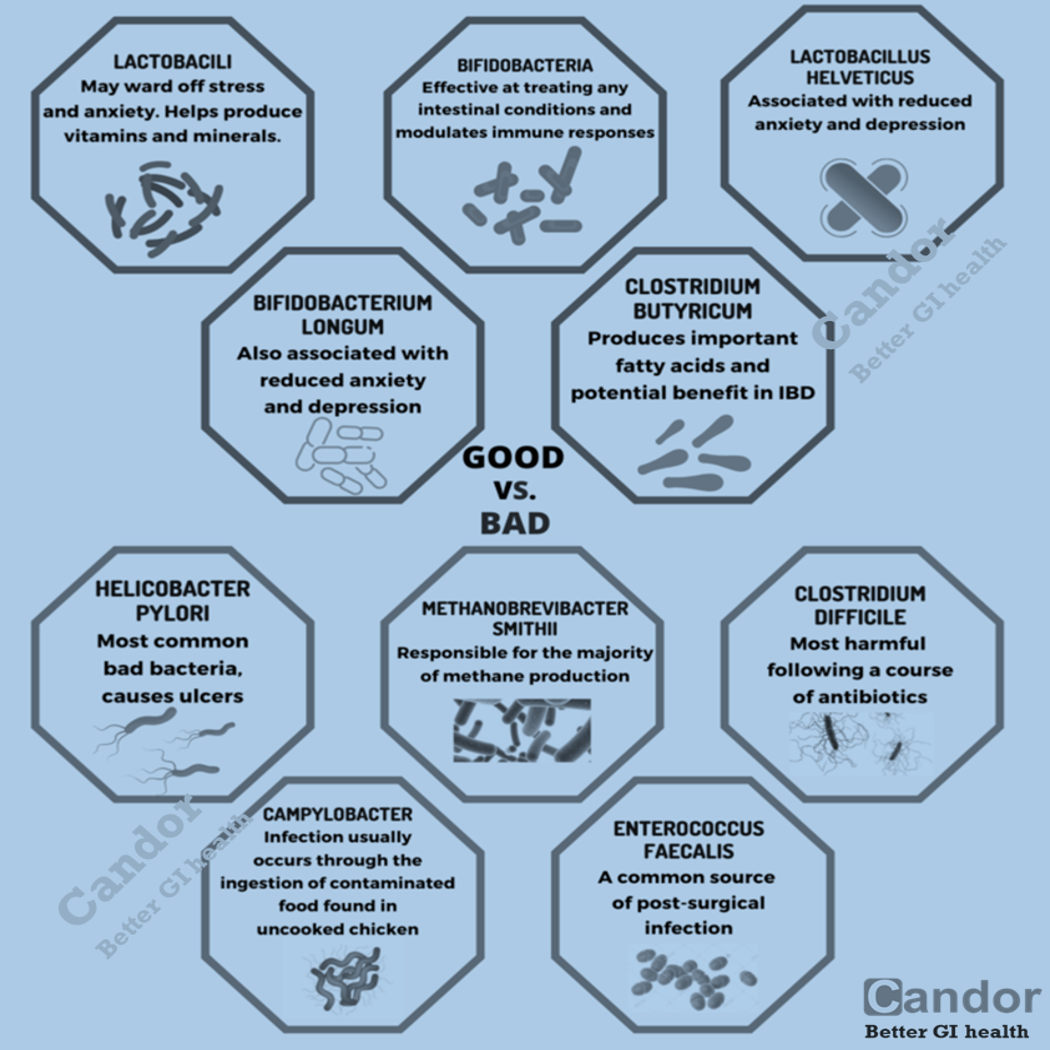
Nevertheless, although FODMAPs can cause certain digestive discomfort in some people, not only do they not cause intestinal inflammation, but they help to prevent it because they produce beneficial alterations in the intestinal flora that contribute to maintain the good health of the colon. FODMAPs are not the cause of irritable bowel syndrome nor other functional gastrointestinal disorders, but rather a person develops symptoms when the underlying bowel response is exaggerated or abnormal.
Fructose malabsorption and lactose intolerance may produce IBS symptoms through the same mechanism but, unlike with other FODMAPs, poor absorption of fructose is found in only a minority. Lactose intolerance is found in a majority of adults with the exception of certain geographic populations, notably those of European descent. Many who benefit from a low FODMAP diet need not restrict fructose or lactose. It is possible to identify these two conditions with hydrogen and methane breath testing and thus eliminate the necessity for dietary compliance if possible.
References:
- Cox SR, Lindsay JO, Fromentin S, Stagg AJ, McCarthy NE, Galleron N, Ibraim SB, Roume H, Levenez F, Pons N, Maziers N, Lomer MC, Ehrlich SD, Irving PM, Whelan K (Jan 2020). “Effects of Low FODMAP Diet on Symptoms, Fecal Microbiome, and Markers of Inflammation in Patients With Quiescent Inflammatory Bowel Disease in a Randomized Trial”. Jounral of Gastroenterology.
- Barrett JS (Mar 2017). “How to institute the low-FODMAP diet”. Journal of Gastroenterology and Hepatology.
- Gibson PR (Mar 2017).”History of the low FODMAP diet”. Journal of Gastroenterology and Hepatology.
- Shepherd SJ, Halmos E, Glance S (Nov 2014). “The role of FODMAPs in irritable bowel syndrome”. Current Opinion in Clinical Nutrition and Metabolic Care.